
National Institute of Allergy and Infectious Diseases, NIH
19 answers referencing 32 sources
Your coronavirus questions, answered by experts
- How long could I have the virus before showing symptoms?
- How does the virus spread between people?
- How can we estimate how far coronavirus will spread?
- How does a virus that apparently started in Wuhan, China spread around the world?
- Do we know why COVID-19 is spreading so much farther compared to related viruses like SARS and MERS?
- What is the difference between coronavirus, COVID-19, and SARS-CoV-2?
- Some "social distancing" explainers — including Massive's — say "stay home." Others say that going outdoors is okay, or even beneficial, as long as people stay >10ft apart. Which is it?
- What percent of the population needs to be infected with coronavirus and recover before herd immunity kicks in?
- How does SARS-CoV-2 get into our cells and can we prevent it from doing so?
- Why are so few people infected in Russia when tens of thousands are sick in China and Europe?
- It seems like cats are also susceptible to COVID-19 but dogs aren't, is there any explanation for that?
- Will UV light, like from the sun, kill coronavirus?
- I've heard people talk about using antibiotics to treat coronavirus. Can you explain why antibiotics don’t work to treat viruses directly?
- Do we know why children are less likely to show severe symptoms?
- How can I infect others if I don't feel sick?
- If one has a normal temperature does that rule out having COVID-19?
- Can a COVID-19 swab test pierce your brain?
- What COVID-19 treatment did President Trump receive? Did it contain human embryonic stem cells?
- Why do the COVID-19 mRNA vaccines need to be kept so cold?
Do you have a different question? Send it to our community of experts:
Submit your questionAre you an expert in this area? Help answer our readers’ questions:
Join our communityHow long could I have the virus before showing symptoms?
TL;DR
The WHO currently estimates the incubation period for COVID-19 to range from one to 14 days, most commonly around five days.

Viruses, like other pathogens, don’t produce symptoms as soon as they come into contact with humans. First, they go through an "incubation period," or a period of time when the virus multiplies to a threshold necessary to produce symptoms in its host. During the incubation period, your body’s immune system recognizes the virus and reacts through multiple kinds of immune responses. If your immune system can keep the virus population in your body below the threshold, you won’t experience symptoms (but may be able to still spread some viruses). The effectiveness of an individual’s immune system in responding to the virus also plays a role — some people can stave off viruses longer than others.
The WHO currently estimates the incubation period for COVID-19 to range from one to 14 days, most commonly around five days (for comparison’s sake, the flu’s incubation period is about two days). However, these estimates could change as we get a better understanding of the disease.
For comparison, the incubation period for measles averages about 10-14 days, but ranges from 7–23 days. The incubation period for SARS is 3-5 days with a range of 2-7 days.
We know that SARS-CoV-2 is spread through person-to-person contact. Specifically, the virus spreads through droplets that form when an infected person coughs or exhales. Sneezing is not a common symptom of COVID19. Those droplets land in the mouths or noses of people who are in close contact (within 6 feet, according to the CDC).
It may also be possible for individuals to become infected with COVID-19 by touching surfaces or objects that has the virus on them (a surface carrying a potential infection is called a “fomite”) and then touching their own eyes, nose, and mouth. A study by scientists at the US National Institute for Allergies and Infections Disease, posted as a pre-print on medRxiv, includes findings that SARS-CoV-2 can persist for up to three days on plastic and steel surfaces.
Airborne transmission has not been reported for COVID-19, and it is not believed to be a major mode of transmission based on available evidence. Typically, airborne transmission describes particles that can suspended in air. Measles and tuberculosis (TB) are examples of airborne viruses. Tiny aerosols can potentially stay in the air for longer and travel further than comparatively large respiratory droplets. The distinction between whether a pathogen can become airborne is thought to depend on its size, however, this is not clear cut.
A feature of infectious diseases that is often cited when examining spread is the basic reproductive number, R0 (pronounced “R-naught”), or the average number of people who will become sick from a single infected person in a population who have never encountered the disease before. If R0 is less than 1, each infection leads to less than one new infection. In this case, the disease will eventually die out. If R0 is greater than 1, each existing infection leads to more than one new infection. The disease will spread between people, and may lead to an outbreak or epidemic.
R0 is used as an indicator of the contagiousness or transmissibility of infectious agents. Early estimates from Wuhan put COVID-19′s R0 at 2.2. This means that, on average, one new case is expected to infect between two and three people in an entirely susceptible population. The R0 for COVID-19 is larger than H1N1 (swine flu), which had an R0 of 1.4-1.6, and is roughly comparable to Ebola (R0 of 1.5-2.5) and SARS (R0 of 2-4). It’s much lower than smallpox (R0 of approximately 6.9), and measles (R0 of 12-18, but with substantial variation). These values tell us COVID-19 is more infectious and easily transmitted than the swine flu, which caused a pandemic in 2009, but less infectious than smallpox and measles.
To further understand virus spread, epidemiologists examine its serial interval, or the duration of time between the onset of symptoms between cases. The serial interval helps identify how cases are related to each other (who infected whom), and can aid in determining appropriate procedures for infection control.
One study in Japan, published in early March, approximated the serial interval for COVID-19 to be about four days, which is shorter than its incubation period. Because COVID-19′s serial interval is shorter than its incubation period, many people are likely spreading it before they even show symptoms.
The incubation period of COVID-19 virus, combined with the possibility that people can possibly spread the disease without showing symptoms, partially explains how the disease spread so widely before being detected.
This incubation period between infection and symptoms allows pathogens to move stealthily across borders before being detected. It is likely that travelers passing through Wuhan were unknowingly encountering people who were infected with SARS-COV-2, the virus that causes the disease known as COVID-19. These travelers may have returned home without knowing they were infected.
Other specific features of SARS-CoV-2 can also help explain how it is making its way around the world, particularly how it moves between people and its infectiousness. We know that SARS-CoV-2 is spread through person-to-person contact and by touching surfaces or objects that has the virus on them.
The World Health Organization has officially declared this outbreak a pandemic and the public health community is continuing to work diligently to further our understanding of this novel disease and to prevent it from spreading. As such, we now must use one of our more stringent methods to slow the spread of this infectious disease and this includes limiting all unnecessary movement and gatherings, including working from home if possible, limiting unnecessary travel, and avoiding large crowds like those at concerts or sporting events.
It is time to approach our daily lives differently. While everyone can’t enact all social distancing measures, individual actions make a big difference. As always: please continue to wash your hands, refrain from touching your face, and stay home if possible. Being prepared is a great way to reduce anxiety and panic.
Do we know why COVID-19 is spreading so much farther compared to related viruses like SARS and MERS?
TL;DR
Most secondary infections from SARS and MERS occurred in hospitals, which prevented community spread of the virus. With COVID-19, we may be seeing more secondary infections and subsequent community spread as a result of primary cases not being tested, either due to lack of tests or lack of severe symptoms.
This is still under investigation, with new data available every day. Beyond features of virus spread, sometimes it is helpful to look at other aspects of a virus to better understand how it behaves.
The case fatality rate (CFR), which is the number of deaths from a given disease divided by the total number of people with confirmed illness, can be used as a measure of disease severity. The global fatality rate for COVID-19 was initially reported as at about 2.3 percent, though WHO reporting has increased this rate to 3.4 percent.
SARS and MERS have higher case fatality rates than COVID-19. The 2003 outbreak of SARS had a case fatality rate of around 10% (774 deaths out of 8098 cases), while MERS has killed 34% of people with the illness between 2012 and 2019 (858 deaths from 2494 cases). However, COVID-19 has lead to more total deaths because more people have been infected.
One hypothesis for the higher case fatality rates with SARS and MERS compared to COVID-19 is related to secondary infections (infections that occur during or after the initial infection). Most secondary infections from SARS and MERS occurred in hospitals, which prevented community spread of the virus. With COVID-19, we may be seeing more secondary infections and subsequent community spread as a result of primary cases not being tested, either due to lack of tests or lack of severe symptoms.
This community spread will continue as we are still having difficulties in identifying and counting mild cases of COVID-19. It currently seems COVID-19 is just as transmissible as SARS and MERS but not as deadly. However, everything we know about the virus, including R0 and case fatality rates, is preliminary and will evolve as the pandemic does.
SARS-CoV-2 is the virus responsible for the novel coronavirus disease. The World Health Organization’s (WHO) chosen name, COVID-19, is just short for "coronavirus disease" and their preferred nomenclature for the virus is "the virus responsible for COVID-19" or "the COVID-19 virus." For readability's sake, Massive often refers to the virus simply as "coronavirus."
Some "social distancing" explainers — including Massive's — say "stay home." Others say that going outdoors is okay, or even beneficial, as long as people stay >10ft apart. Which is it?
TL;DR
If you are not sick, going outside is fine if you maintain distance from other people. If you are ill, stay inside.
Last updated
Answered by
-
![]()
Bioethics, Public Health, and Biochemistry
Columbia University

Walking, hiking, running, and bicycle riding outdoors is fine as long as people stay at least 6 feet apart. The city of San Francisco, which is currently under an order “Requiring Residents Stay at Home Except for Essential Needs” makes an explicit exemption for engaging in individual outdoor activities. Exercising outdoors is also much safer than going to the gym. This is because the virus will not stay concentrated in the air outdoors, unlike in enclosed indoor spaces, where it may remain in the air or settle on hard surfaces.
In times of emergency, public health authorities must communicate clearly to large populations all at once. In this case, the safest mass message has been “stay home,” because this is the clearest way to communicate that people should avoid parties, sporting events, and other large gatherings of people. What might get lost in this message is that going outside in areas where people are not gathered is fine. In fact, one of the reasons many viruses such as influenza tend to infect people seasonally in the winter is that people are more likely to be gathered in closed environments during that time.
But, if you are sick or are feeling symptoms (fever, coughing, and shortness of breath in particular), stay home.
What percent of the population needs to be infected with coronavirus and recover before herd immunity kicks in?
TL;DR
It's too early to give an accurate figure. If you absolutely must have a number, 66% is a very preliminary, very rough estimate.
Last updated
Answered by
-
![]()
Bioethics, Public Health, and Biochemistry
Columbia University
Herd immunity refers to the protection that an at-risk individual can gain by being surrounded by others who are already immune to a disease. It relies on a proportion of individuals within a population already having immunity to an infection, but the exact proportion of individuals needed for herd immunity depends on the characteristics of each particular infection. In addition, the understanding of the concept has been developed mainly as related to vaccination, where immunity is produced in a person by giving a vaccine, rather than that person having to develop and recover from the disease. This is important for understanding the need for widespread measles vaccination, because measles can spread quickly through a population if fewer than 93-95% of people are vaccinated. In addition, moving from one population to another can change an individual’s level of protection, since different groups often have different characteristics and levels of immunity.
How easily an infection is transmitted is measured by the “basic reproductive number” or R0 of the virus. This can be defined as “Number of secondary cases generated by a typical infectious individual when the rest of the population is susceptible (i.e., at the start of a novel outbreak).”
The current estimate of the R0 for the virus that causes COVID-19 is 2.79, meaning that 1 infected person will on average infect 2.79 others. A rough estimate based on an R0 of 3 results in 66% percent of people needing to have immunity before there is any “herd” immunity effect for the population. But this estimate is based on incomplete information, and there is evidence that the R0 might actually be higher than currently estimated. Many individuals who had minor symptoms have not been tested for the virus, so they have not been counted in the total infection numbers. Individuals in China who tested positive who did not have symptoms also may not have been counted in the number totals for “confirmed cases.” These factors would mean that our current estimates are misleading and that the proportion of immune individuals needed for herd immunity might actually be higher than we currently estimate.
Recently, the UK discussed a potential strategy for that country based on herd immunity, but it has since been discarded and they have now implemented strict controls similar to other countries. This "herd immunity" approach, if sustained, would have resulted in a huge number of deaths, not only from coronavirus cases, but also of other individuals who could no longer access needed hospital or medical supplies in a system overwhelmed by coronavirus.
There are some additional uncertainties about this virus that could impact the possibility of herd immunity. First, there were early reports that individuals might not develop immunity as expected, and that reinfection may be possible, but scientists find this unlikely and say the apparent reinfection is probably due to testing error or to the virus staying in some people's bodies for a longer time, leading to a second flare-up of the same disease. Finally, viral evolution may impact immunity in unknown ways. Influenza strains shift rapidly because of mutation and the tendency for genetic material to “re-assort,” or move between viral strains, even within the infected host. This means that seasonal influenza vaccines must be targeted to include likely strains every year. There is evidence that this novel coronavirus is also mutating into multiple strains, but it is unclear what difference this might make over time for population immunity.
How does SARS-CoV-2 get into our cells and can we prevent it from doing so?
TL;DR
The virus is covered in a “spike protein” that attaches strongly to a different protein (ACE-2) found at the surface of some human cells. After attaching, the virus can enter the cell and replicate freely. Some researchers think we can halt this process by preventing the virus from attaching in the first place. That would require tinkering with the levels of ACE-2, or potentially

SARS-CoV-2, like its relative SARS, is covered in tiny protein “spikes,” or S-Proteins. Those spikes are the key to getting the virus to infiltrate our otherwise healthy cells. But, despite their name, the spike proteins don’t poke and slash a path into any human cell — the actual process is far more elegant.
It turns out that the S-Protein attaches really well to a different protein that dots the outside of some of our cells. That protein, the angiotensin converting enzyme 2, or ACE2, sits on the surface of some cells in our lungs, and other organs like the kidney and heart. The coronavirus recognizes that protein through an interesting biochemical interaction. The ACE2 protein at the surface of some human cells is shaped like a sort of claw and regions of negative charge. The viral S-Protein, on the other hand, is suggested to have key regions of positive charge that attach well to ACE2.
Ultimately, when people are exposed to the virus, either through contaminated coughs or face-touches, the virus can sneak into their airways and latch on to the ACE2 on healthy cells – many of which are in the lungs. The attached SARS-CoV-2 then gets absorbed into the cell and releases its cargo: a short fragment of genetic code.
The cell reads this genetic code, a blueprint for its own self-destruction, and builds all the bits and pieces for the coronavirus to copy itself. The infected cell basically turns into a coronavirus factory. This is how one virus particle turns into billions and makes you sick.
Many possible anti-viral drugs aim to target the virus’ ability to copy itself. But a COVID-19 treatment doesn’t have to focus only on viral replication. We may also see successful drugs that go after completely different aspects of coronavirus infection. After the 2003 outbreak of SARS, researchers showed that cells react to coronavirus infections by reducing the amounts of ACE2 available for the virus to latch on to. That may sound like a good thing, but our bodies may rely on ACE2 to protect us from organ damage.
Outside of this pandemic, ACE-2 is an important regulator of blood pressure. High ACE-2 activity triggers the body to dilate blood vessels.
One proposed treatment currently in trials uses losartan, a blood pressure and diabetes medication. Losartan increases the levels of ACE2, the protein that the virus’ spike proteins target, and can prevent lung damage from COVID as a result. These ever-important ACE2 levels may even contribute to why the elderly are more susceptible to severe infections, as ACE2 levels appear to decrease with age.
Other studies using compounds that affect levels of ACE2, such as Vitamin D, have researchers wondering whether this strategy could help treat COVID. But limited scientific data is available to support these claims so far.

It's hard to say without speculating. But, Russia and the USSR before it have a long, long history of suppressing news or recasting unflattering figures. For instance, this January Russia reported a 37% increase in "pneumonia," one of the primary symptoms of COVID-19, compared to 2019. But it appears an outbreak is growing there too.
It's not really possible to explain different species' experience with coronavirus with much certainty right now. You might have seen the news about a tiger at the Bronx Zoo being infected, but there have been a few reports of house cats infected. It's unclear if any dogs have been infected as well.
Based on some very early studies of coronavirus, you can make some guesses, but that's all they'd be. For instance, a recent paper determined how coronavirus's spike protein latches on to a protein on the surface of cells, called ACE2, that it uses as a door to enter cells and replicate. Here's a picture of the spike protein and ACE2 together, with the interface between them circled:
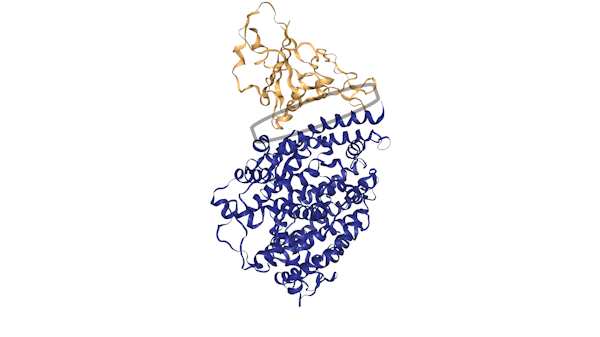
A picture of the human ACE2 protein and the spike protein from SARS-CoV-2 (coronavirus) interacting. The spike protein is in white, ACE2 in blue.
PDB 3SCI
Humans, cats, and dogs all have ACE2 receptors, but they differ a bit, with several of those differences occurring in the region between where the spike protein contacts ACE2 (if you want to look at the sequences yourself you can download them here). The dog version, for instance, is missing a tiny portion (one amino acid) of ACE2 that humans and cats have near the region of contact with coronavirus.
But there is no way to know right now if that's what matters. I emailed Sarah McDonald, a virologist at Wake Forest University to ask about ACE2. She said: "In theory, YES, one amino acid change at a KEY site in ACE2 is enough to prevent productive binding by the viral spike."
But McDonald stressed it's simply too soon to know anything for certain. "There are LOTS of factors/variables that determine whether an animal host gets infected with a given virus. [Similarity between ACE2 receptors] is just ONE factor. For instance, it is possible that dogs don’t express the ACE2 receptor at high enough levels on their cell surface; low receptor = low or no infection. It is alternatively possible that the dog receptor is just fine and it mediates attachment/entry [of the virus]....but maybe the dog cells lack a critical...factor preventing viral replication. Elucidating the mechanism of host [reaction to] this new coronavirus will take YEARS of research."

The answer is UV light probably would inactivate the virus, but there's no medical guideline for how much exposure and how long it would take, and we have other methods that are sure to work (like soap). UV is used as a sterilizing agent in a number of procedures, and if you're somewhere water may not be of the highest quality, approximately 5-6 hours in the sun in a clear bottle is a good rule of thumb. That said, people should still definitely be wearing sunscreen out and about because the damage from UVA/UVB is likely to be worse than any benefit it would provide. Now putting things like nonperishable groceries, the mail, in a sunny spot for 24 hours like I have heard of a number of people doing? If you are using good hand hygiene, that's probably sufficient, and it won't hurt anything, so sure, go ahead. This logic also applies to disinfecting public places of coronavirus as well.
Now, you may have seen UV used to disinfect money/buses/medical equipment. Those are particularly strong UVC lights (shortwave UV almost entirely scattered in the atmosphere) that can be incredibly damaging to the skin. This kind of UV disinfection is reserved for industrial processes.
I've heard people talk about using antibiotics to treat coronavirus. Can you explain why antibiotics don’t work to treat viruses directly?
TL;DR
Antibiotics work in ways that are specific to bacterial infections and do not work for viruses because bacteria and viruses are very different in structure and activity.
Last updated
Answered by
-
![]()
Bioethics, Public Health, and Biochemistry
Columbia University
Bacteria are typically single-celled organisms that live almost everywhere on earth, both outside of and inside of other organisms. Antibiotics treat infection by disrupting specific bacterial features and processes. For example, penicillin interrupts the process through which certain types of bacteria construct and maintain the cell wall, which then kills the bacterium. Not all bacteria are identical, and different antibiotics work in different ways, making some effective only for limited types of bacterial infections.
Viruses, on the other hand, are not cells and must infect another organism in order to survive and reproduce, and for this reason, most biologists do not consider viruses to be fully alive. Different types of viruses can infect all types of living organisms, including animals, plants, and even bacteria.
Antivirals are used to treat viruses by destroying the viral structure, inhibiting the viral entry into host cells, or preventing the virus from reproducing. Not only is it ineffective to treat a virus with an antibiotic, it can also be dangerous. Some bacteria have grown resistant to antibiotics through evolution, which makes medical treatment of infection more and more difficult. For this reason, overuse of antibiotics over time has resulted in a global crisis of antibiotic resistance.
It is possible that an opportunistic bacterial infection will occur when a person is already ill with a viral infection. An important example is the tendency for tuberculosis bacteria to infect individuals already infected with the HIV virus. There is also a risk of opportunistic bacterial infections secondary to the viral COVID-19 infection, but since our experience with this virus is still new, the full scope and details are not yet clear. In cases of opportunistic bacterial infection, antibiotic treatment may be needed, but whenever possible, it is best to first have confirmation of the bacterial infection through testing in order to avoid unnecessary side effects and to prevent the development of antibiotic resistant bacterial strains.
Scientists currently do not know why children are less likely to develop severe symptoms (persistent high fever, severe cough, shortness of breath, and extreme body ache) if infected with SARS-CoV-2, the virus that causes COVID-19. The Centers for Disease Control and Prevention (CDC) noted that while some children and infants have been sick with COVID-19, adults make up most of the known cases to date.
Initial data from more than 72,000 cases of COVID-19 in Wuhan, China showed that just 2% of the infected cases were under the age of 19. Similarly, a February report from the World Health Organization’s (WHO) mission to China showed that those under 18 accounted for only 2.4% of the infected. Out of those infected young people, 2.5% developed severe disease and 0.2% developed critical disease.
While we don’t know why children are less likely to show severe symptoms, researchers are trying to understand how children experience COVID-19. They see some distinctions in symptom presentation between children and adults who are infected with SARS-CoV-2. A retrospective analysis of 366 hospitalized children in Wuhan, China, from January 7 to January 15, 2020 found SARS-CoV-2 in 6 patients (1.6%). All six children experienced high fever (>39°C, > 102.2°F ) and cough, and four of the six children had pneumonia, as assessed by x-ray. However, another analysis of 10 Chinese children infected with SARS-CoV-2 found their chest X-rays lacked definite signs of pneumonia, one defining feature of infection in adults.
A study in the journal Pediatrics of more than 2,100 children in China found that children of all ages were vulnerable to COVID-19, regardless of biological sex, though the vast majority experienced mild symptoms, and some experienced none at all. This is different from what we are seeing emerge from COVID-19 infection rates in adults, as scientists have begun to see more men than women becoming infected, and a higher proportion of infected men dying in Italy and China.
Data on COVID-19 cases among U.S children was published by the CDC in a Morbidity and Mortality Weekly Report (MMWR). As of April 2, 2020, 149,082 cases of COVID-19 were reported for which age was known, and 2,572 (1.7%) occurred in children under 18 years. For reference, children under the age of 18 account for 22% of the U.S. population. Reported symptoms of COVID-19 among children in the US are a lot like those of children in other countries in that pediatric patients reported fever, cough, and shortness of breath, though less frequently than adults (73% of children reported symptoms compared to 93% of adults 18-64 reporting at least one of these symptoms). Data on child’s biological sex was known for 2,490 pediatric cases and 1,408 (57%) COVID-19 cases occurred in males, a finding that has been seen in adults as well. Reasons for any potential sex differences in COVID-19 cases remains unknown and requires further research.
While our current research indicates COVID-19 does occur in children, scientists have yet “... to determine the extent of infection among children, what role children play in transmission, whether children are less susceptible or if they present differently clinically (i.e. generally milder presentations).” It also remains unknown as to whether children with underlying medical conditions and special healthcare needs are at higher risk for severe illness. As this is an ongoing pandemic of a brand new disease, there is more to learn about how the disease impacts children. An important factor is how many children are being tested for the virus, because without this data it’s hard to gauge the rate of infection and severe illness for children in the US.
To date, we understand SARS-CoV-2 to be spread from person-to-person through respiratory droplets when people are in close contact (within about 6 feet). It is also possible for individuals to become infected with SARS-CoV-2 by touching surfaces or objects that has the virus on them (a surface carrying a potential infection is called a “fomite”) and then touching their own eyes, nose, and mouth. Whether you feel sick or not, you can spread COVID-19 through these routes.
We have learned from research in Japan that individuals can spread the virus before they feel sick because the serial interval of COVID-19 (the duration of time between the onset of symptoms between serially-linked cases) is shorter than its incubation period, which suggests many people are likely spreading it before they even show symptoms. Further research found infectiousness may begin 2 to 3 days before the appearance of the first symptoms. This means that even if you do not feel sick but are infected with the virus (whether you know it or not), you can still spread the virus by touching surfaces after coughing on your hands or breathing or coughing on people in close proximity to you.
The Director of the Centers for Disease Control and Prevention (CDC), Dr. Robert Redfield, recently suggested that as many as 25 percent of people infected with the SARS-CoV-2 may not show symptoms. This high percentage of infected individuals without symptoms means it is hard to predict COVID-19 spread as well as strategies to mitigate its impact. Understanding the spread of COVID-19 by asymptomatic (not exhibiting symptoms) and presymptomatic (the period before symptoms have developed) individuals may help explain why COVID-19 set off a pandemic in a way that the SARS and MERS viruses did not.
Current research suggests that you can infect people and become infected with SARS-CoV-2 without having symptoms, so having a normal temperature does not rule you out from having COVID-19. In fact, early research showed that as few as 31% of passengers on Diamond Princess cruise ship who tested for COVID-19 had a fever at diagnosis.

No, a swab can't poke a hole in your brain. even if it feels like the swab is all the way into your head. News stories about piercing the brain during a COVID test are generally due to a rare weak spot or defect at the base of a skull. According to nose surgeon Carl Philpott, "It is extremely unlikely for any person who doesn’t have this pre-existing weakness in the nose to cause any damage with a swab."
When President Donald Trump was sick with COVID-19, he immediately received an experimental polyclonal antibody cocktail made by Regeneron, a large biopharma company. As of October 2020, this treatment had not yet been evaluated by the FDA.
Despite rumors circulating online, the antibodies were developed using "humanized" mouse embryonic stem cells. The treatment does not contain human cells.
Read more about the experimental treatment in our full story.
Why do the COVID-19 mRNA vaccines need to be kept so cold?
TL;DR
Two vaccines are RNA-based, and RNA is notorious for its instability. Cold temperatures slow down the degradation.
Last updated
Answered by
-
Biological Engineering
Massachusetts Institute of Technology

Pfizer-BioNTech’s vaccine requires -70°C (-94°F), colder than the South Pole, and only lasts around 5 days once placed in a refrigerator. Moderna’s vaccine is a bit more forgiving, shipped at -20°C (-4°F) and good for a month in a refrigerator. For comparison, inactivated or live attenuated vaccines (like the flu vaccine) are stored at typical refrigerator temperatures, about 2-8°C (46°F).
Both of these vaccines are RNA-based. Instead of priming the immune system with a dead virus or a piece of a virus, as vaccines in the past have done, these vaccines deliver a template – RNA – for our cells to make a single protein from SARS-CoV-2. The body creates the protein, generates a protective immune response, then throws away the RNA – much like kids passing notes in class, then crumpling them up and tossing them in the trash.
RNA is notorious for its instability. Before working with RNA, it’s common for scientists working with it in a lab to clean their workspace of “RNases” or ubiquitous environmental enzymes that break down RNA quickly. Unlike DNA, which typically consists of two strands and contains a submolecule called deoxyribose (hence “DNA”), RNA is single-stranded and contains ribose (hence “RNA”), which makes RNA molecules more susceptible to degradation. Despite the chemical modifications and packaging these companies use to make it more resistant, it still suffers compared to DNA or protein.
The extreme temperatures slow down chemical and enzymatic degradation, allowing the RNA vaccines to maintain their efficacy from manufacturing to injection. RNA’s instability is good for our cells: many copies of RNA are transcribed from DNA templates, which are then used to create proteins. But as the proteins required by the cell are made, the instructions are degraded away.
Read more about the cold requirements and the cold supply chain in this story.